Cephalometry Techniques for Diagnosis & Treatment Planning
Cephalometry is a cornerstone in orthodontic diagnosis and treatment planning, enabling precise assessment of craniofacial relationships. This page delves into the systematic approach of cephalometric analysis, guiding practitioners through the process of tracing cephalograms and identifying critical anatomical landmarks. By mastering these techniques, clinicians can enhance their diagnostic accuracy, leading to more effective and personalized orthodontic interventions.

1. Trace Cephalogram First
Use a pencil and a lightbox or software.
2. Anatomical Points
-
The midpoint of the sella turcica, a saddle-shaped depression in the sphenoid bone where the pituitary gland is located. This signifies where “growth is initiated from” in the head and neck complex. This is a stable point which does not move. This is also the posterior point of the cephalometric cranial base, which is stable and can be used as a reference point to which other measurements are related.
-
It is the most anterior point of the frontonasal suture, located on the skull's frontal bone. This point is an important landmark in cephalometric analyses and is commonly used in conjunction with other points, like the Sella (S), to form the S-N line, which serves as a baseline for many angular measurements evaluating craniofacial growth patterns, anteroposterior skeletal relationships, and other aspects of craniofacial morphology.
-
It is the most anterior point on the curvature of the maxilla, specifically at the maxillary alveolar ridge. The "A point" is commonly used in conjunction with other cephalometric landmarks to assess the anteroposterior relationship between the maxilla and mandible, as well as to determine facial growth patterns and the position of the maxilla relative to the cranial base or other structures. One common measurement that utilizes the "A point" is the ANB angle, which involves the "A point", "Nasion", and "B point" to assess the sagittal relationship between the upper and lower jaws.
-
It is the most anterior point on the curvature of the mandible, specifically at the mandibular alveolar ridge. The "B point" is commonly used in cephalometric analyses alongside other landmarks to evaluate the anteroposterior relationship of the mandible in relation to the maxilla and other craniofacial structures. One of the most frequent measurements that incorporates the "B point" is the ANB angle, which includes the "A point", "Nasion", and "B point". The ANB angle helps in determining the sagittal relationship between the maxilla and mandible.
-
It is the tip or the most posterior point of the bony projection at the junction of the palatine bones on the roof of the mouth, marking the rear of the nasal floor or the posterior limit of the nasal cavity. The PNS is often used in conjunction with other cephalometric points for various measurements to assess the skeletal and dental relationships in the craniofacial region, particularly those related to the maxilla and the nasal cavity. It's crucial for analyses that involve the vertical and anteroposterior positioning of the maxilla.
-
It is the tip or the most anterior point of the bony projection of the upper jaw (maxilla) located at the base of the nasal cavity. The ANS, along with the Posterior Nasal Spine (PNS), helps in defining the length of the maxillary palate and is commonly used in various cephalometric analyses. Measurements involving ANS can provide information about the vertical and anteroposterior dimensions and relationships of the maxilla in relation to other craniofacial structures.
-
It is the most anterior point on the bony chin's contour, located on the symphysis of the mandible. The Pogonion (Pog) is frequently used in cephalometric analyses to assess the anteroposterior position and projection of the chin, especially in relation to other craniofacial landmarks. It's vital for evaluating the profile aesthetics and determining the nature of skeletal malocclusions.
-
It is the most inferior point on the mandibular symphysis, which is the lowest point of the chin on the outline of the mandible. The Menton (Me) is a significant landmark used in various cephalometric analyses to assess vertical facial dimensions, growth patterns, and the position of the mandible relative to other craniofacial structures.
-
It is the most anteroinferior point on the bony contour of the chin. It's essentially the point where the lower border of the mandible meets the midline of the chin. The Gnathion (Gn) is frequently used in cephalometric analyses to assess the vertical and anteroposterior position and growth pattern of the mandible, especially in relation to other craniofacial landmarks.
-
It is the point located at the curvature or bend of the angle of the mandible, where the ascending ramus and the lower border of the mandible meet. The Gonion (Go) is a key landmark used in many cephalometric analyses. It helps in evaluating the shape, position, and growth pattern of the mandibular ramus and the mandible as a whole, especially in relation to other craniofacial structures.
-
This is the most inferior point of the bony eye socket (the lowest point on the margin of the orbit). The Orbitale (Or) is utilized in various cephalometric analyses, especially when assessing vertical facial relationships and dimensions. It can be used in conjunction with other cephalometric points to derive meaningful linear and angular measurements for diagnostic and treatment planning purposes. It forms the anterior point of the Frankfurt Horizontal Plane.
-
Po which is the uppermost point on the external ear canal's margin or the external auditory meatus. It is the posterior part of the Frankfurt Horizontal Plane.
Included Points:
Incisor Superioris (often just termed 'Incisal' for the upper incisor):
i. Is: The incisal edge or tip of the maxillary (upper) central incisor.
ii. U1: The labial surface of the crown of the upper central incisor, often used to represent the inclination of the tooth.
iii. U1 root apex: The apex of the root of the maxillary central incisor.
Incisor Inferioris (often just termed 'Incisal' for the lower incisor):
iv. Ii: The incisal edge or tip of the mandibular (lower) central incisor.
v. L1: The labial surface of the crown of the lower central incisor, commonly used to determine the inclination of the tooth.
vi. L1 root apex: The apex of the root of the mandibular central incisor.



3. Anatomical Planes
-
The Frankfurt Horizontal Plane, often simply referred to as the Frankfurt Plane, is an anatomical reference plane used in both anthropology and cephalometry. It was established at an anthropological congress held in Frankfurt, Germany in 1884 and has since become a standard cranial reference plane. The Frankfurt Plane is defined by a straight line connecting two anatomical landmarks:
i. Porion (Po): The uppermost point on the external auditory meatus (ear canal).
ii. Orbitale (Or): The most inferior point on the margin of the eye socket (orbit).
When a skull or a head is oriented such that the Frankfurt Plane is horizontal, it's considered to be in the anatomical position. This standardized orientation is particularly useful for comparative studies, ensuring that measurements and observations are consistent across different subjects. In orthodontics and cephalometry, the Frankfurt Plane can be one of the reference lines used to assess craniofacial angles and relationships.
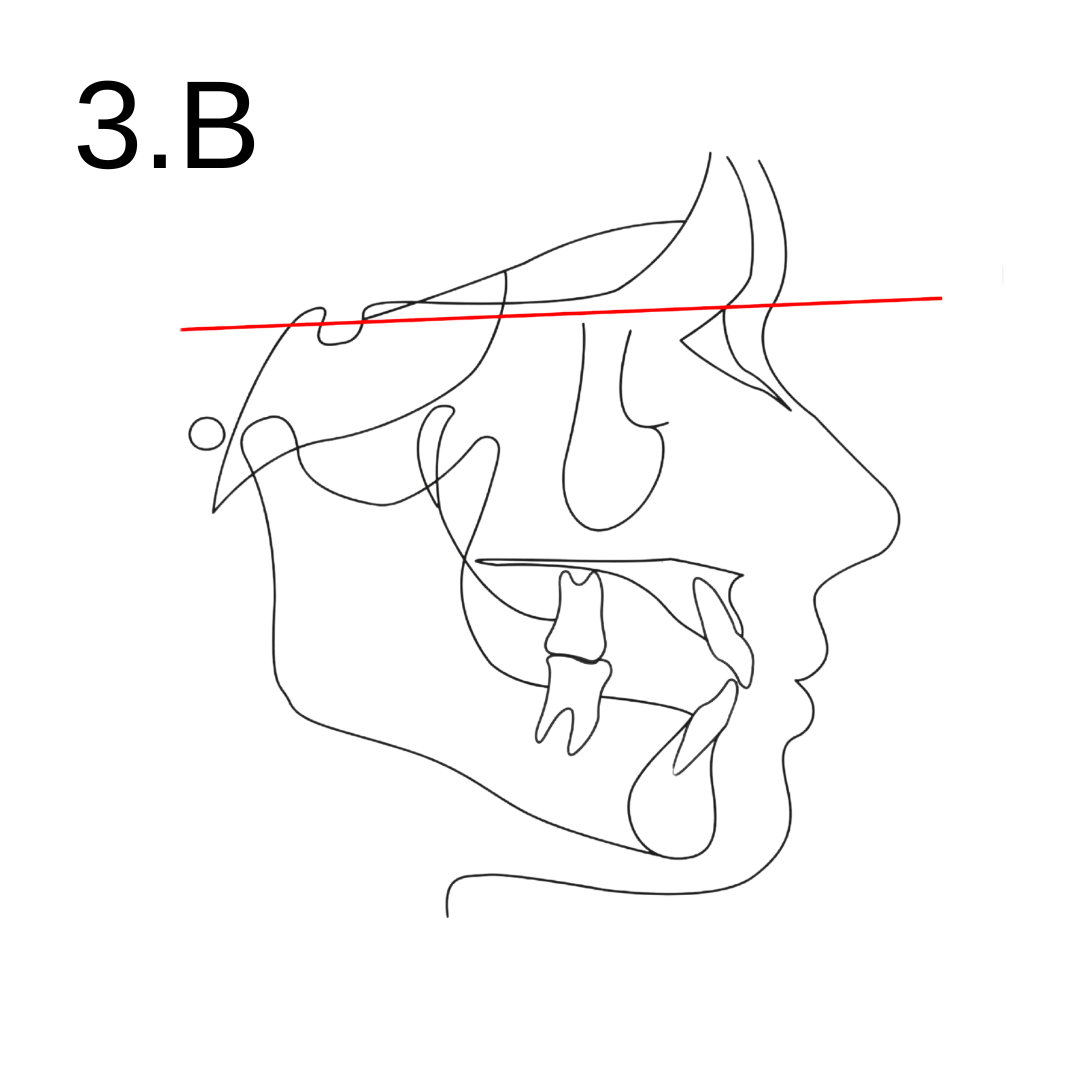
-
The S-N plane, often simply referred to as the SN plane or the sella-nasion line, is a commonly used anatomical reference plane. It's defined by a straight line connecting two significant cranial landmarks:
i. Sella (S): The midpoint of the sella turcica, a saddle-shaped depression in the sphenoid bone where the pituitary gland is located.
ii. Nasion (N): The most anterior point of the frontonasal suture, located on the frontal bone of the skull.
The SN plane serves as a baseline in many cephalometric analyses and signifies the cranial base. Various angles and distances relative to this plane are used to determine the anteroposterior and vertical relationships of facial structures, assess growth patterns, and plan orthodontic or orthognathic surgical treatments. The orientation and position of the maxilla, mandible, and teeth can be analyzed in relation to the SN plane.
-
The NA plane (or NA line) is a linear reference constructed by connecting two essential cranial landmarks:
i. Nasion (N): The most anterior point of the frontonasal suture, located on the frontal bone of the skull.
ii. A Point (Subspinale, or simply A): The most anterior point on the curvature of the maxilla, specifically at the maxillary alveolar ridge.
The NA line is used in various cephalometric analyses to assess the anteroposterior position of the maxillary alveolar base.
-
The NB plane (or NB line) is a linear reference constructed by connecting two significant cranial landmarks:
i. Nasion (N): The most anterior point of the frontonasal suture, located on the frontal bone of the skull.
ii. B Point (Supramentale, or simply B): The most anterior point on the curvature of the mandible, specifically at the mandibular alveolar ridge.
The NB line is instrumental in various cephalometric analyses to evaluate the anteroposterior position of the mandibular alveolar base.
-
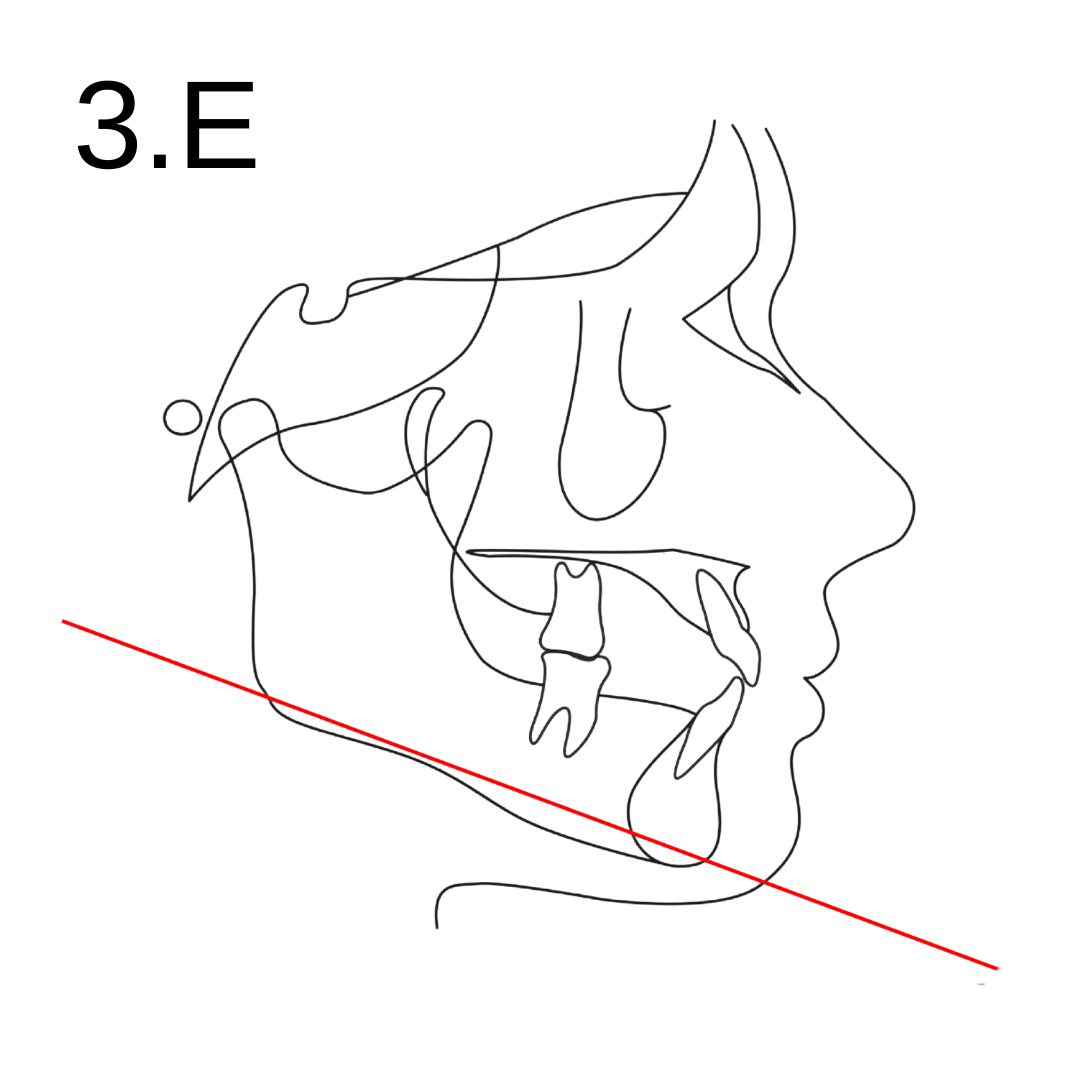
The mandibular plane is an essential reference line used to assess the vertical relationship and growth pattern of the mandible. It's defined by a straight line connecting two anatomical landmarks:
i. Gonion (Go): This point is located at the curvature or bend of the angle of the mandible, where the ascending ramus and the lower border of the mandible meet.
ii. Gnathion (Gn): The most anteroinferior point on the bony contour of the chin.
The angle formed between the mandibular plane and other reference planes, such as the Frankfurt Horizontal plane or the S-N plane, can provide information about the vertical growth pattern of an individual. For example: A larger-than-average angle between the mandibular plane and the Frankfurt Horizontal or S-N plane may indicate a "high angle" growth pattern, often associated with an open bite tendency and a longer lower facial height. Conversely, a smaller-than-average angle may indicate a "low angle" growth pattern, often linked with a deep bite tendency and a shorter lower facial height.
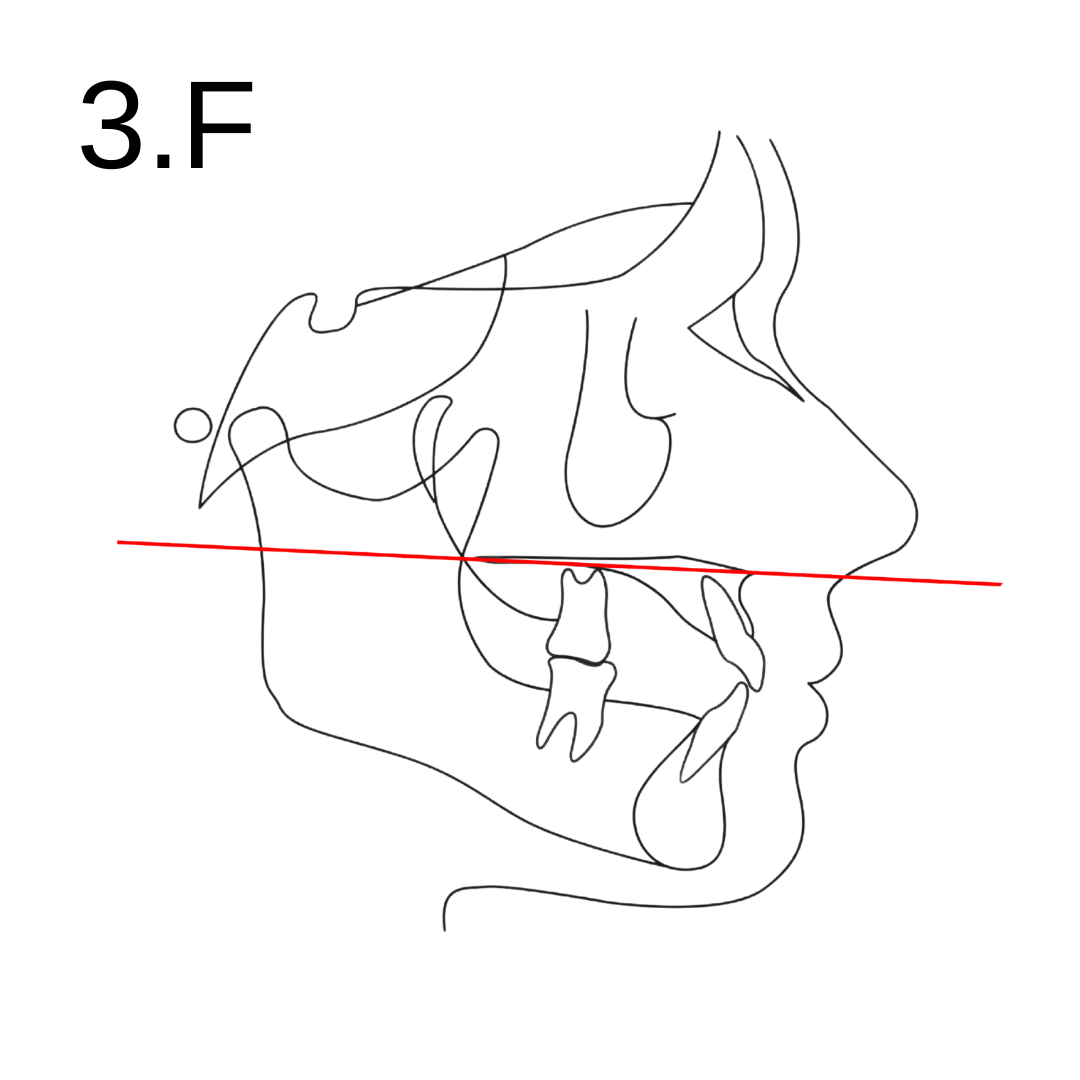
-
The maxillary plane is a reference line used to assess the position and orientation of the maxilla. It's defined by a line connecting two anatomical landmarks:
i. Anterior Nasal Spine (ANS): The most anterior point of the bony nasal spine of the maxilla.
ii. Posterior Nasal Spine (PNS): The most posterior point of the bony nasal spine of the maxilla.
The line connecting ANS and PNS forms the maxillary plane, often referred to as the "ANS-PNS line" or "palatal plane." This plane is crucial in cephalometric analyses to evaluate the vertical and anteroposterior position of the maxilla. The orientation of the maxillary plane relative to other cranial planes, like the cranial base or mandibular plane, provides insights into the overall facial morphology and potential growth patterns. The maxillary plane can also be used to assess the inclination of the maxillary teeth, especially when analyzing the angulation of the upper incisors relative to this plane. This is important for orthodontic treatment planning, especially in cases involving significant vertical discrepancies or anteroposterior maxillary discrepancies.
-
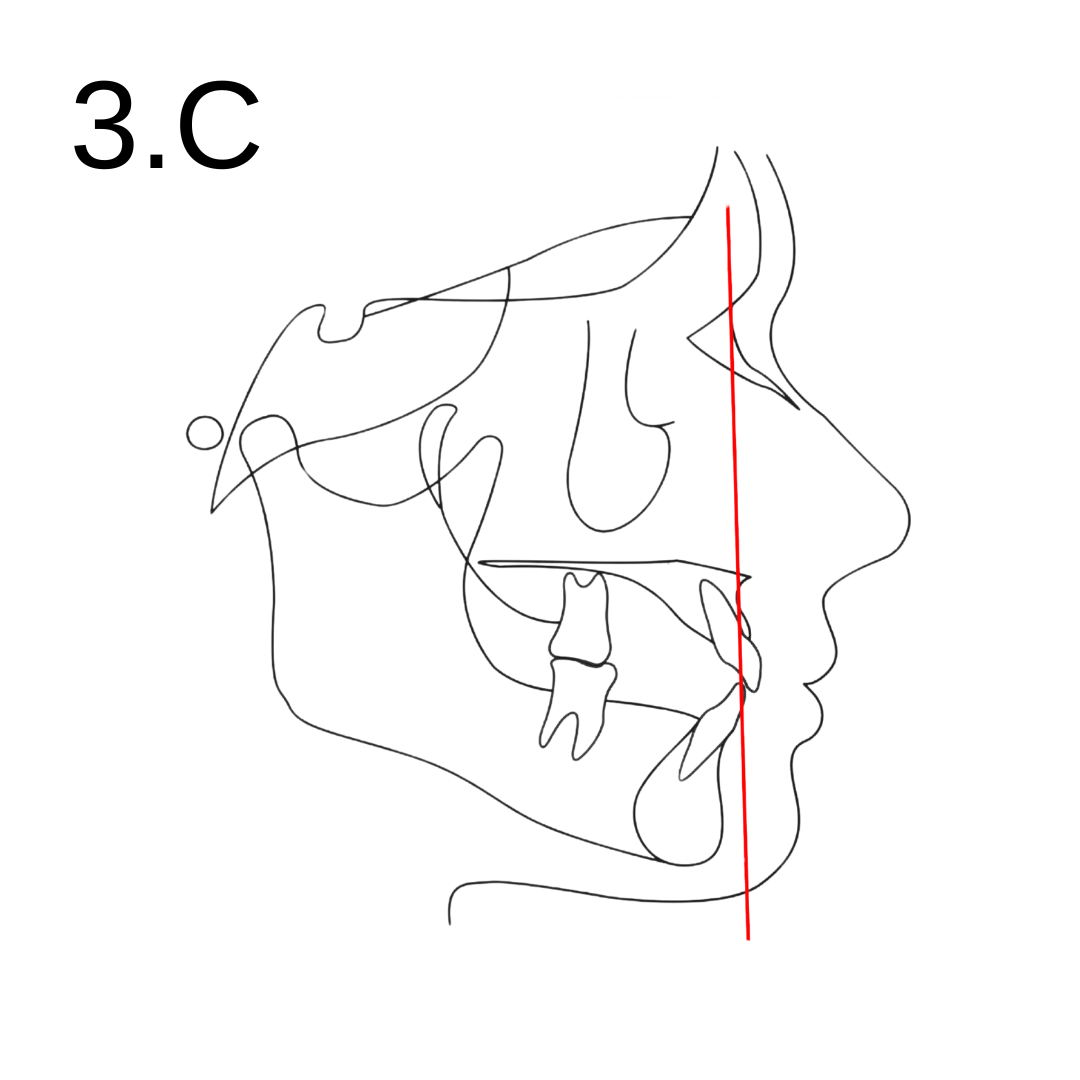
The "upper incisor long axis" refers to the long axis or the midline of the crown and root of the maxillary central incisor. This line can be used to determine the inclination or angulation of the upper incisor in relation to other reference planes. Here's how the upper incisor long axis is commonly assessed:
i. One point on this line is the incisal edge of the maxillary central incisor, often termed "UI" (Upper Incisor) or "Is" (Incisor superioris).
ii. The second point is typically the root apex of the maxillary central incisor.
When this line (the upper incisor long axis) is drawn on a cephalometric radiograph, it can be compared to other reference planes, such as:
NA Plane: To determine the angulation of the upper incisor relative to a standard skeletal reference line.
Maxillary Plane (ANS-PNS): To assess the incisor's inclination concerning the maxillary or palatal plane.
-
The "lower incisor long axis" refers to the long axis or the midline of the crown and root of the mandibular central incisor. This line is used to determine the inclination or angulation of the lower incisor in relation to other cephalometric reference planes. Here's how the lower incisor long axis is typically defined:
i. One point on this line is the incisal edge of the mandibular central incisor, often termed "LI" (Lower Incisor) or "Ii" (Incisor inferioris).
ii. The second point is the root apex of the mandibular central incisor.
When this line (the lower incisor long axis) is drawn on a cephalometric radiograph, it can be compared to other reference planes, such as:
NB Plane: To determine the angulation of the lower incisor relative to a standard skeletal reference line.
Mandibular Plane (Go-Gn): To assess the incisor's inclination concerning the mandible's lower border.



4. Important Angles
-
The SNA angle is one of the most commonly used angular measurements to evaluate the anteroposterior position of the maxilla relative to the cranial base. Here's a breakdown of the SNA angle:
i. Sella (S): The midpoint of the sella turcica, a saddle-shaped depression in the sphenoid bone where the pituitary gland resides.
ii. Nasion (N): The most anterior point of the frontonasal suture, located on the frontal bone of the skull.
iii. A Point (Subspinale, or simply A): The most anterior point on the curvature of the maxilla, specifically at the maxillary alveolar ridge.
The SNA angle is formed by drawing lines from Sella to Nasion and from Nasion to A Point. This angle typically measures between 80° and 82° in Caucasian populations, though there is variation based on individual and ethnic differences. An increased SNA angle indicates a forward (anterior) position of the maxilla relative to the cranial base, often termed as "maxillary prognathism." Conversely, a decreased SNA angle suggests a posterior or retrusive position of the maxilla, commonly referred to as "maxillary retrognathism." Evaluating the SNA angle is vital for understanding the skeletal basis of malocclusions and for treatment planning in orthodontics and orthognathic surgery.
-
The SNB angle is a fundamental angular measurement used to assess the anteroposterior position of the mandible relative to the anterior cranial base. Here's a breakdown of the SNB angle:
i. Sella (S): The midpoint of the sella turcica, a saddle-shaped depression in the sphenoid bone where the pituitary gland is located.
ii. Nasion (N): The most anterior point of the frontonasal suture, located on the frontal bone of the skull.
iii. B Point (Supramentale, or simply B): The most anterior point on the curvature of the mandible, specifically at the mandibular alveolar ridge.
The SNB angle is formed by drawing lines from Sella to Nasion and from Nasion to B Point. This angle typically measures between 78° and 80° in Caucasian populations, though, like other cephalometric measurements, there can be variation based on individual and ethnic differences. An increased SNB angle indicates a forward (anterior) position of the mandible relative to the anterior cranial base, often referred to as "mandibular prognathism." Conversely, a decreased SNB angle suggests a posterior or retrusive position of the mandible, commonly termed "mandibular retrognathism." The SNB angle, in combination with the SNA angle (which assesses maxillary position), is instrumental in evaluating the skeletal relationship between the maxilla and mandible, aiding in the diagnosis and treatment planning of orthodontic and orthognathic cases.
-
The ANB angle is a fundamental cephalometric measurement used to assess the anteroposterior (AP) skeletal relationship between the maxilla and the mandible. It provides an indication of whether a patient has a skeletal class I, II, or III relationship.
Here's a breakdown of the ANB angle:
i. A Point (Subspinale, or simply A): The most anterior point on the curvature of the maxilla, specifically at the maxillary alveolar ridge.
ii. Nasion (N): The most anterior point of the frontonasal suture, located on the frontal bone of the skull.
iii. B Point (Supramentale, or simply B): The most anterior point on the curvature of the mandible, specifically at the mandibular alveolar ridge.
The ANB angle is formed by subtracting the SNB angle from the SNA angle. In other words, it's the angle between the NA line and the NB line at point Nasion. Typically, the ANB angle values are as follows (though there can be variation based on individual and ethnic differences):
iv. Class I: ANB angle between 2° and 4°
v. Class II: ANB angle greater than 4° (indicating the maxilla is positioned anteriorly relative to the mandible or vice-versa)
vi. Class III: ANB angle less than 2° or negative (indicating the mandible is positioned anteriorly relative to the maxilla)
The ANB angle is a key measurement in orthodontic diagnosis and treatment planning. However, it's worth noting that it's just one of many measurements used to evaluate a patient's skeletal and dental relationships. Furthermore, some criticisms surround the ANB angle, mainly due to potential changes in the Nasion position with growth, which can influence the measurement. As a result, clinicians often use it in conjunction with other cephalometric and clinical assessments.
-
The FMPA (Frankfort Mandibular Plane Angle) is a cephalometric measurement that represents the angle between the Frankfurt Horizontal Plane and the Mandibular Plane. It is used to assess the vertical growth pattern and facial morphology of a patient. Here's a breakdown of the FMPA:
i. Frankfurt Horizontal (FH) Plane: A plane established by connecting two anatomical landmarks:
1. Porion (Po): The uppermost point of the external auditory meatus or ear canal.
2. Orbitale (Or): The lowest point on the infraorbital rim.
ii. Mandibular Plane: A plane typically represented by a straight line connecting:
1. Gonion (Go): The point located at the curvature of the angle of the mandible where the ascending ramus and the lower border of the mandible meet.
2. Gnathion (Gn): The most anteroinferior point on the bony contour of the chin.
The FMPA is the angle formed between the Frankfurt Horizontal Plane and the Mandibular Plane. FMPA is valuable in orthodontic assessments because: A higher FMPA (or increased angle) often indicates a hyperdivergent growth pattern, which may be associated with an open bite tendency and a longer lower facial height. A lower FMPA (or decreased angle) indicates a hypodivergent growth pattern, often linked with a deep bite tendency and a shorter lower facial height. Evaluating the FMPA aids orthodontists in diagnosing vertical discrepancies, understanding facial growth patterns, and formulating appropriate treatment plans, whether orthodontic or orthognathic in nature.
-
The MMPA (Mandibular to Maxillary Plane Angle) is a cephalometric measurement used to assess the vertical relationship between the maxillary and mandibular planes, which in turn helps in determining the vertical facial growth pattern of a patient. Here's a breakdown of the MMPA:
Maxillary Plane (also called Palatal Plane): A line connecting the:
i. Anterior Nasal Spine (ANS): The most anterior point of the bony nasal spine of the maxilla.
ii. Posterior Nasal Spine (PNS): The most posterior point of the bony nasal spine of the maxilla.
Mandibular Plane: A plane typically represented by a straight line connecting:
iii. Gonion (Go): The point located at the curvature of the angle of the mandible where the ascending ramus and the lower border of the mandible meet.
iv. Gnathion (Gn): The most anteroinferior point on the bony contour of the chin.
The MMPA is the angle formed between the Maxillary (or Palatal) Plane and the Mandibular Plane. Assessing the MMPA provides valuable insights because: A higher MMPA indicates a hyperdivergent growth pattern, which may be associated with increased vertical facial growth and potentially an open bite tendency. A lower MMPA indicates a hypodivergent growth pattern, often linked with decreased vertical facial growth and potentially a deep bite tendency.
-
The angle between the upper incisor long axis and the maxillary (or palatal) plane is a significant measurement used to assess the inclination of the maxillary incisors relative to the maxillary skeletal base. This angle provides information about the positional relationship of the upper front teeth to the underlying skeletal structures, helping in diagnostic and treatment planning processes.
Here's a breakdown:
i. Maxillary (or Palatal) Plane: A reference line connecting the:
1. Anterior Nasal Spine (ANS): The most anterior point of the bony nasal spine of the maxilla.
2. Posterior Nasal Spine (PNS): The most posterior point of the bony nasal spine of the maxilla.
ii. Upper Incisor Long Axis: A line representing the midline or long axis of the crown and root of the maxillary central incisor. It typically starts at the incisal edge and extends through the root apex of the incisor.
The angle formed between the upper incisor long axis and the maxillary (or palatal) plane is often termed the "Upper Incisor to Maxillary Plane Angle" or "U1 to Maxillary Plane Angle" (where U1 denotes the upper first incisor). Clinically, this angle helps to:
Determine the inclination of the maxillary incisors: Proclined (forward-tilted) or retroclined (backward-tilted) relative to the maxillary skeletal base. Formulate treatment plans: Especially in cases that may require orthodontic tooth movement, extractions, or orthognathic surgery. The ideal value for this angle varies among different cephalometric analyses and populations. However, a commonly referenced norm for the upper incisor inclination to the maxillary plane is approximately 110°, though individual and ethnic variations exist.
-
The angle between the lower incisor long axis and the mandibular plane is an important measurement used to evaluate the inclination of the mandibular incisors relative to the mandibular skeletal base. This angle offers insights into the positional relationship of the lower front teeth to the underlying bone and plays a crucial role in diagnosis and treatment planning. Here's a detailed explanation:
i. Mandibular Plane: A line typically connecting the:
1. Gonion (Go): The point located at the curvature of the angle of the mandible where the ascending ramus and the lower border of the mandible meet.
2. Gnathion (Gn): The most anteroinferior point on the bony contour of the chin.
ii. Lower Incisor Long Axis: A line representing the midline or long axis of the crown and root of the mandibular central incisor. It usually starts at the incisal edge and extends through the root apex of the incisor.
The angle between the lower incisor long axis and the mandibular plane is often termed the "Lower Incisor to Mandibular Plane Angle" or "L1 to Mandibular Plane Angle" (where L1 represents the lower first incisor). Clinical significance of this angle: Determine the inclination of the mandibular incisors: An increased angle may indicate proclined (forward-tilted) incisors, while a decreased angle suggests retroclined (backward-tilted) incisors relative to the mandibular base. Assist in treatment planning: Knowing the inclination is vital when considering orthodontic treatments such as tooth movement, extractions, or even orthognathic surgery. Typically, the normative value for the inclination of the lower incisor to the mandibular plane is around 90° to 95°, but it's essential to consider individual variations and other clinical factors. The exact ideal angle can also vary depending on the specific cephalometric analysis being used and the ethnic or individual characteristics of the patient.
-
The inter-incisor angle, in the context of orthodontic cephalometry, refers to the angle formed between the long axes of the upper (maxillary) and lower (mandibular) central incisors. This measurement provides insights into the inclination or tilt of the front teeth in relation to each other. Here's a breakdown:
i. Upper Incisor Long Axis: A line representing the long axis of the crown and root of the maxillary central incisor. This line typically starts at the incisal edge and extends through the root apex of the incisor.
ii. Lower Incisor Long Axis: A line representing the long axis of the crown and root of the mandibular central incisor, also extending from the incisal edge through the root apex.
The angle formed between these two axes is the inter-incisor angle. Clinical relevance of the inter-incisor angle: Evaluate Incisor Inclination: It helps assess whether the incisors are proclined (tilted forward) or retroclined (tilted backward) in relation to each other. For instance, a larger inter-incisor angle may suggest that the maxillary incisors are proclined or the mandibular incisors are retroclined or a combination of both.
Treatment Planning: The information from this angle aids in formulating orthodontic treatment plans, especially when considering the esthetic and functional position of the incisors.
Post-Treatment Evaluation: It can also be used to evaluate changes in incisor position after orthodontic treatment or to monitor the stability of treatment results.
Normative values for the inter-incisor angle can vary, but a common reference is around 130° to 140°. It's crucial to consider individual variations and ensure the angle facilitates a proper overjet and overbite relationship while maintaining esthetic and functional outcomes.








5. Super Impositions
Cephalometric superimpositions are a technique used in orthodontics and dentofacial orthopedics to evaluate the skeletal and dental changes that occur over time in a patient. By superimposing cephalometric radiographs taken at different times onto a stable anatomical structure, orthodontists can visualize and measure the changes in tooth and bone position. This is especially useful for tracking the effects of orthodontic treatment, growth modifications, or orthognathic surgery. The process of superimposition involves overlaying two or more cephalometric tracings to compare changes between different time points. There are various regions in the cephalogram where superimpositions can be made based on the structures being analyzed:
a. Cranial Base Superimposition: Used to assess overall facial growth and the effects of orthodontic treatment or surgical interventions on the maxilla and mandible. Commonly done by matching the structures of the interior cranial base, especially around the sella turcica and along the contour of the anterior cranial base.
b. Maxillary Superimposition: Used to evaluate changes in the maxilla and the upper teeth. Superimposed on the best fit of the palatal plane or other stable structures like the zygomatic crest or anterior nasal spine (ANS).
c. Mandibular Superimposition: Used to assess changes in the mandible and the lower teeth. Depending on the age of the patient and the structures of interest, superimposition can be done on the inner cortical outline of the symphysis or along the inferior border of the mandible.
d. Dental Superimposition: Used to assess tooth movement specifically. Done by overlaying the images on stable dental structures such as the palatal contour for maxillary teeth and the contour of the mandibular canal for mandibular teeth.
After the superimposition process, the clinician can then analyze the differences between the tracings to determine the direction and magnitude of changes. This information is invaluable in understanding the progress of treatment, making future treatment decisions, and assessing growth patterns.
6. Classification
Analysis fundamentally relies on angles and distances as its core elements. These measurements, whether in degrees or millimeters, can be perceived as either fixed or relative values. They can also be compared to understand proportional relationships.
Different types of analyses include:
· Angular Analyses: Focuses on angles.
· Linear Analyses: Concerned with distances and lengths.
· Coordinate Analyses: Uses Cartesian coordinates, sometimes expanding into 3-D dimensions.
· Arcial Analyses: Uses arcs for comparative studies.
These methods can be categorized based on the principles that determine standard values:
· Mono-normative Analyses: Utilizes averages as standards. These could be arithmetic (mean values) or geometric (mean tracings). An example is the Bolton Standards.
· Multi-normative Analyses: Incorporates a range of standards, considering factors like age and gender. Bolton Standards is an example.
· Correlative Analyses: Evaluates individual facial differences to understand their interrelationships. The Sassouni arcial analysis is one such example.
7. Other Analyses
Other common analyses used in cephalometry include the following:
· Modified Eastman Analysis (as above)
· Down’s Analysis
· Tweed’s Analysis
· Witt’s Analysis
· Sassouni Analysis
· Harvold Analysis
· Macnamara Analysis
· Jarabak Analysis
· Rickett’s Analysis
· Bjork’s Analysis
· Steiner’s Analysis